Sight is arguably one of our most important senses. We rely upon it to navigate through our surroundings with ease. Loss of vision can have a huge impact on a person’s life, but many disorders that cause blindness are currently difficult or impossible to treat. Researchers are now using stem cell technology to explore possible new approaches to treatments for loss of vision.
What do we know?
Treatments for most disorders that cause vision loss are difficult or not yet possible.
Specialised cells in the eye serve specific functions. These include focusing light, and transforming light into signals which get sent to the brain. The eye contains several different types of stem cells that constantly replace these specialised cells as they become worn out or damaged.
Holoclar® is currently the only clinically approved stem cell treatment for the eye. This treatment restores vision to patients with damaged corneas: the clear, outermost part of the eye. This treatment works by transplanting lab-grown limbal stem cells into areas of the eye lacking these cells.
What are researchers working on?
Holoclar® only works if patients have some limbal stem cells left in their eyes for clinical labs to grow. New methods of making limbal cells with pluripotent stem cells are being developed for patients without any limbal stem cells left.
Researchers are studying how transplants of retinal pigment epithelial cells made with pluripotent stem cells might prevent vision loss in patients with diseases such as age-related macular degeneration (AMD). For more advanced AMD, researchers are working on generating light-sensitive cells for transplantation.
Researchers are also using stem cells to study many different aspects of the eye, such how the eye develops, what causes eye diseases, and how to treat them.
What are the challenges?
Many diseases that cause blindness and vision deterioration are still not treatable. Researchers are working to understand what causes these diseases, what other types of stem cells reside in the eye and how stem cells might be used to repair or even restore vision in patients. Many of these studies are still in the early years. Holoclar® took more than twenty years to develop into a safe and successful treatment; today’s research and discoveries will take time to develop into safe, reliable treatments for other types of blindness.
Cell and gene therapies: paths to treating blindness
Did you know that some people can see a larger range of colours due to a rare genetic mutation? This condition, known as tetrachromacy, allows individuals to possess an extra type of cone cell in their eyes, providing enhanced colour perception beyond the normal range experienced by most people.
Eye diseases encompass a wide range of conditions affecting vision. These include myopia, hyperopia, cataracts, glaucoma, and age-related macular degeneration (AMD). Stem cell therapy holds promise for restoring vision by replacing damaged or lost cells in the eye.
Stem cells can potentially differentiate into specialized retinal cells, such as photoreceptors or retinal pigment epithelium (RPE) cells. By transplanting these cells, researchers aim to repair or regenerate the damaged tissues and preserve sight.
Continued research and clinical trials are underway to explore the potential of stem cell therapies for various eye diseases. Currently, there is only one approved stem cell therapy for vision disorders: Holoclar®, which uses stem cells from the eye to repair corneal damage.
About the eye
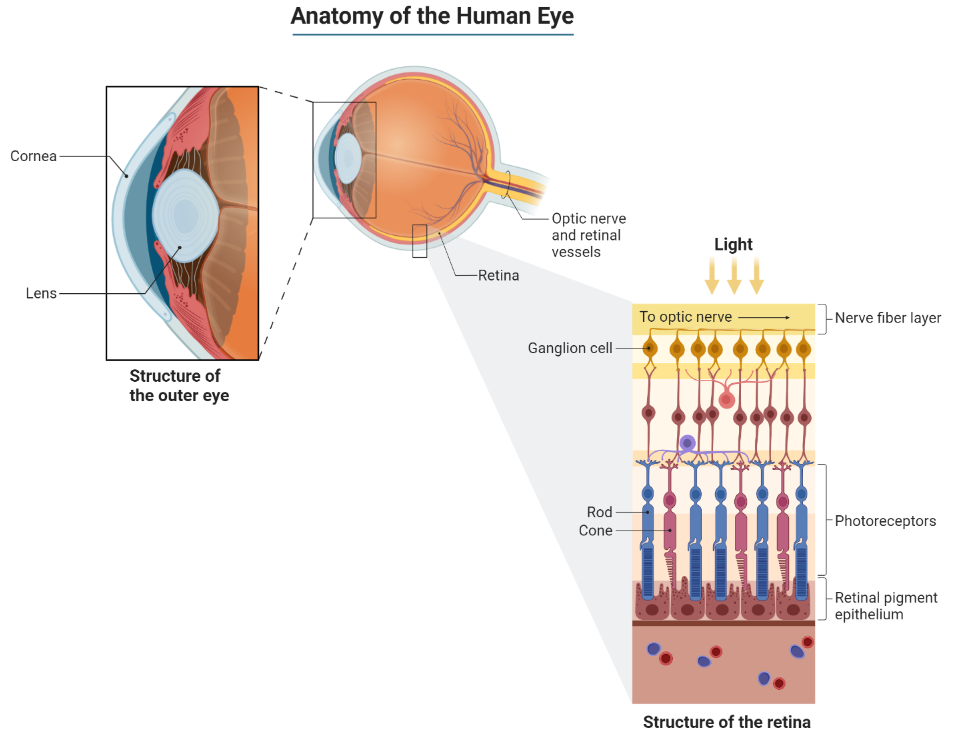
The eye is the organ responsible for our ability to see the world around us. It detects light from the surrounding environment, and transfers information about what it has detected to the brain.
The eye is a very complex organ made up of multiple, specialized components, not unlike an electronic camera. The components, or tissues, are comprised of several types of cells. Each cell type has a specific job, which enables the tissues to perform their specialised roles.
The eye is a complex organ made up of multiple layers of different cell types
The main parts of the eye are:
Cornea
The transparent ‘window’ on the front of the eye. This acts as a protective outer layer and helps focus incoming light on the retina.
Lens
A clear, flexible structure located behind the iris (the coloured part of the eye). This acts just like a lens in a camera by focusing the light that enters the eye.
Retina
The ‘electrical circuit’ at the back of the eye that is responsible for seeing. It is the most complex component of the eye. It is made up of several different types of cells with specific roles. These include photoreceptor cells, which detect the light entering the eye and produce an electrical signal in response.
Optic nerve
A biological ‘wire’ that connects the eye to the brain. It is responsible for transferring the electrical signal produced by photoreceptors from the retina to the brain. The brain then interprets this signal to give us a picture of our environment. The optic nerve is closely associated with the retina.
Retinal pigment epithelium
A sheet of black cells that sit beneath the retina. This sheet supports the retina and has several important roles, including processing nutrients and removing waste products.
Disorders or diseases of the eye occur when one or more of these components is damaged or stops working properly. Different disorders develop depending upon which component(s) are not working. The difficulty in treating these problems is that new biological components for the eye are not easy to obtain. This is where stem cell technology may be of use. Stem cells can act as a source of new, healthy specialised cells, and may provide a way to replace damaged cells in the eye. There are several types of stem cells that could be used in different ways, depending upon the specific disorder. So, what is current research focused on?
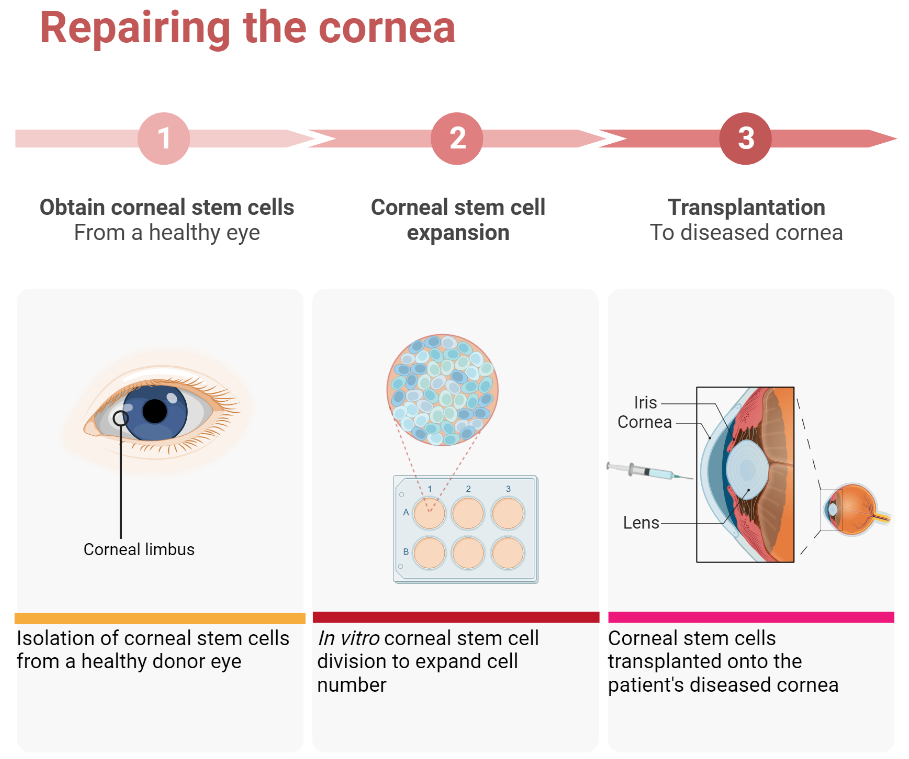
Repairing the cornea
Cells that make up the cornea (the window part of the eye) are constantly damaged by blinking and exposure to the outside world. To repair this damage, we have a small number of stem cells at the edge of the cornea, known as limbal stem cells. They are responsible for making new corneal cells to replace damaged ones. If these stem cells are lost due to injury or disease, the cornea can no longer be repaired. This affects the ability of light to enter the eye, resulting in a significant loss of vision.
Following many years of painstaking research, scientists have now developed a technique which uses limbal stem cells [define] to repair the cornea. These cells are collected from a healthy donor eye, or from a region of the patient’s own eye which still has healthy limbal cells. They are grown in large numbers in the lab, then transplanted into the damaged eye.
Clinical trials have shown that transplantation of limbal stem cells from a healthy eye can repair the cornea and permanently restore vision. To avoid immune rejection, this treatment only works if the patient has a healthy section of limbus from which to collect the limbal stem cells.
Repairing the cornea:Currently the only stem-cell-based therapy for the eye that has been proven to work in clinical trials.
At present, this is the only available stem cell treatment in the eye that has been proven by clinical trials to work. In 2015, the European Commission gave authorization (following approval by the European Medicines Agency) for an advanced therapy medical product (ATMP) containing limbal stem cells to be marketed to healthcare providers. This is the final step in the clinical translation process happening after successful clinical trials. The combined gene and cell therapy, called Holoclar®, is based on more than twenty years of excellence in research, conducted by a team of internationally renowned scientists in the field of epithelial stem cell biology. It is produced in GMP (Good Manufacturing Practice)-certified facilities in line with European legislation, by an Italian University spin-out company called Holostem Terapie Avanzate S.r.l and commercialised by Chiesi Farmaceutici S.p.a.
Holoclar® represents a personalized and regenerative approach to address limbal stem cell deficiency. It's essential to consult an ophthalmologist or corneal specialist to determine eligibility for this therapy.
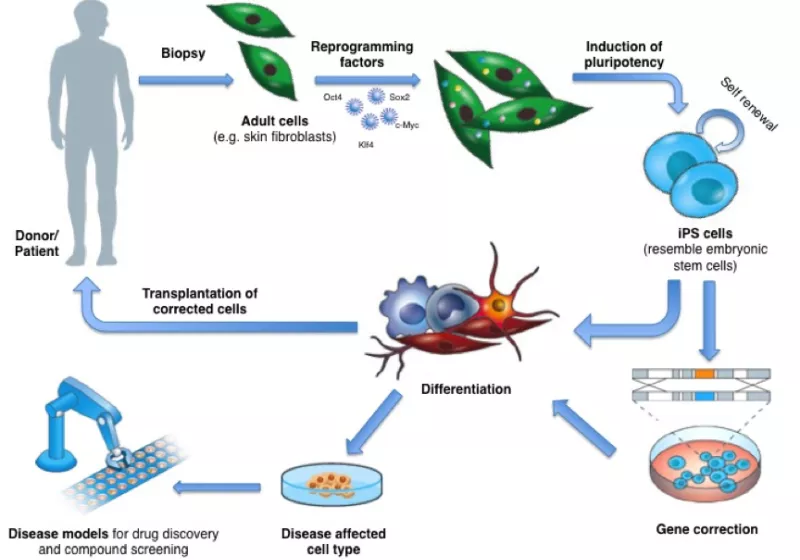
If the corneas of both eyes are badly injured (bilateral limbal deficiency), this therapy will not work. This is because there are no residual limbal stem cells available to collect. Researchers are currently investigating the possibility of using a different approach. This involves using embryonic stem cells, induced pluripotent stem (iPS) cells, or oral mucosa stem cells to make new limbal stem cells in the lab. This could remove the need for complex surgery to collect limbal stem cells. It could also provide a theoretically endless source of limbal stem cells for patients who require new ones.
Retinal dystrophy
Retinal dystrophy is a group of genetic conditions which cause damage to the light-sensing membrane at the back of the eye (the retina). Light-sensing cells (photoreceptors), are damaged in these conditions. This abruptly stops the conversion of light into electrical signals, meaning that visual information is not sent to the brain. These conditions, such as retinitis pigmentosa, cone-rod dystrophy, and macular dystrophy, often worsen over time. This leads to a progressive loss of vision.
Retinal dystrophies are caused by genetic mutations which are inherited in different patterns. While there is no cure for most of these conditions, ongoing research aims to slow disease progression and restore function through treatments like gene therapy and cell-based therapies. Early diagnosis and monitoring are essential for managing retinal dystrophies.
One gene therapy, Luxturna (authorised by the EMA for use in Europe in 2018), targets a specific gene (RPE65). Mutations in this gene cause Retinitis Pigmentosa and Leber’s Congenital Amaurosis. One of the challenges that remain for this therapy is that it can only be used when there are still a suitable number of healthy cells remaining in the retina.
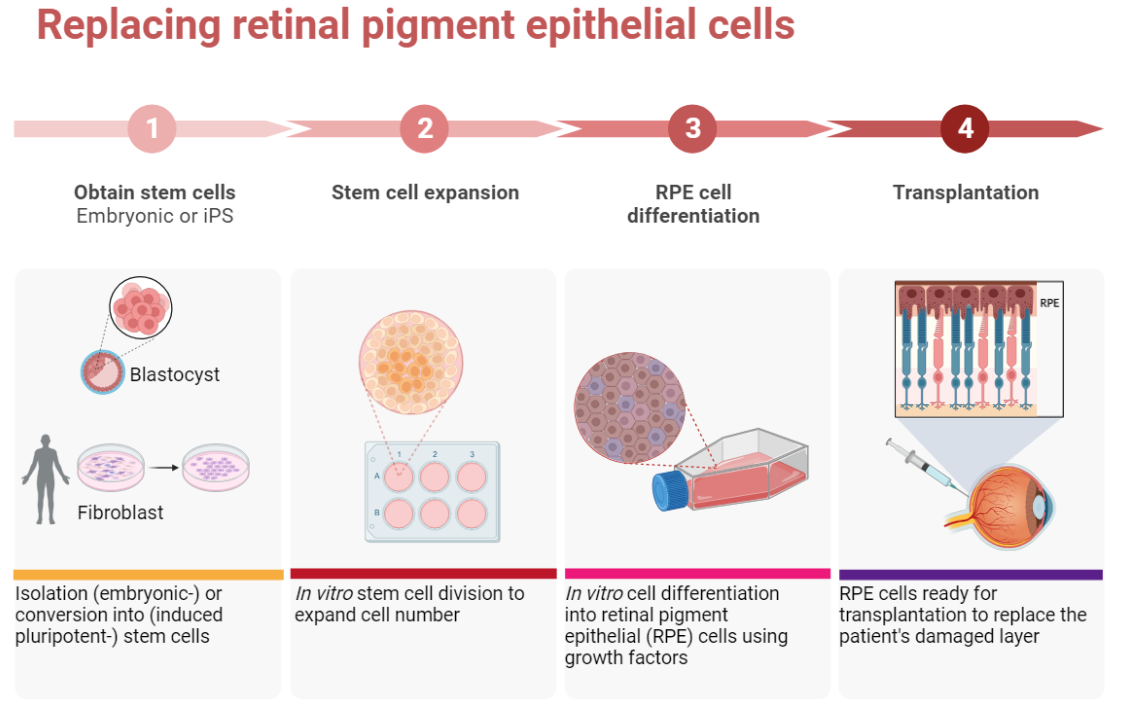
Retinal pigment epithelial (RPE) cells have several important jobs. These include looking after the adjacent retina. If RPE cells stop working properly due to damage or disease, certain parts of the retina die. As the retina is responsible for detecting light, this leads to the onset of blindness. RPE cells can be damaged in a variety of diseases, such as age-related macular degeneration (AMD), retinitis pigmentosa, and Leber’s congenital amaurosis, amongst others.
One way to treat these diseases would be to replace the damaged RPE cells with transplanted healthy cells. Unfortunately, it is not possible to take healthy RPE cells from donors. This is why it is necessary to find another source of cells for transplantation.
The pioneering transplantation of foetal human RPE cells into the subretinal space of AMD patients without immunosuppression began in 1997. In recent years, scientists have been able to produce new RPE cells in the lab, using both embryonic stem cells and iPS cells in the lab. Several of these studies are in the early stages of clinical trials (Phase 1/Phase 2 trials). This means that extensive effort is being put towards establishing the safety, and secondarily the effectiveness, of pluripotent stem cell-derived RPE cells.
One of such trial focussed on the safety of embryonic stem cell-derived RPE cells for patients with Stargardt’s macular dystrophy and AMD. The results of the trial, published in 2014, demonstrated that this treatment was safe for use. It also showed engraftment of the transplanted RPE cells (that is, integration of the transplanted cells into the patients’ own tissue). However, some participants experienced adverse side effects from the both the immunosuppression and the transplantation procedure itself. Several patients also reported an improvement in vision, even though this was not the goal of this trial. (At this stage, the end goal is determining safety.).
Another study in 2015 also used RPE cells derived from human ESCs to treat patients with AMD. The two patients in this trial experienced significant improvements to their vision. [In support of this study, the benefits of human embryonic stem cell-derived RPE s for wet AMD were explored in another phase I/II clinical trial in the United Kingdom. This work, initiated with the first patient receiving their transplant in September 2015, was led by Prof Peter Coffey and Lyndon da Cruz and was carried out at Moorfields Eye Hospital as part of the London Project to Cure Blindness. Using an engineered patch of RPE cells, the two patients included in the trial reported significant improvements to their vision.]
Dr Masayo Takahashi initiated the world’s first clinical study of RPE cells made from iPS cells in 2014. This treatment was trialled on a single patient with AMD. The study showed that the cells integrated into the patient’s own tissue with no adverse effects. [This clinical trial focussing on wet AMD reported maintained engraftment and survival of the transplanted autologous iPSC-derived RPE sheet beneath the retina as well as exhibiting slight expansion of the pigmented area with no adverse events, in the one patient included.]There are several other early-stage clinical trials using pluripotent stem cells. These all involve small numbers of participants. These trials are investigating treatments for both types of AMD (dry and wet), as well as Stargadt’s macular degeneration. Additional clinical trials investigate alternative cell therapies and their benefits, such as using mesenchymal stem cells.
One of the main challenges of cell replacement therapy for retinal dystrophies is that, as the disease progresses, transplants become less successful. Replacement of damaged RPE cells will only be effective in patients who still have at least part of a working retina, and therefore some level of vision. This means that it needs to take place in the early stages of the disease). This is because the RPE cells are not themselves responsible for ‘seeing’ but are instead responsible for supporting the ‘seeing’ retina.Sight is lost in these types of diseases when the retina begins to degenerate because the RPE cells are not doing their job properly. This means that the RPE cells need to be replaced in time for them to support a retina that is still working. Scientists hope that that transplantation of new RPE cells will then permanently halt further loss of vision, and in some cases may even improve vision.
Replacing retinal pigment epithelial cells: Techniques for growing cells for therapies are being researched and tested in early clinical safety trials.
Replacing retinal cells
The first successful therapy for any eye disease was the use of 'anti-VEGF' drugs in the early 2000s for wet age-related macular degeneration (AMD).
When vision is lost over time, the problem often lies with malfunctioning retinal circuitry. Different disorders occur when specialised cells in the circuit either stop working properly or die off. Although the retina is more complicated than other components of the eye, scientists hope that that if a source of new retinal cells can be found. This may enable them to replace the damaged or dying cells to repair the retina. In addition, this approach may also help to repair damage caused to the optic nerve.
Scientists have turned to stem cell technology to source replacement cells. Several studies have reported that both embryonic stem cells and iPS cells can be turned into different types of retinal cells in the lab.
Within the eye, certain retinal cells (Müller glia cells) can encourage regeneration of damaged tissue within the retina. However, this is only true of some animals (such as zebrafish), and is not true in mammals. In recent years, efforts are being put into investigating a new technique called in vivo cell fusion. This involves fusing Müller glia cells with adult stem cells to form a type of cell hybrid. These hybrid cells have shown promising results in terms of their ability to differentiate into other retinal cell types. Scientists are investigating whether these cells might be used to repair the damaged retina.
RPE cell transplantation can only be used in patients who still have some functioning retinal cells. However, is it possible that direct repair of the retina could be used in treating patients who have already lost their vision. These technologies may be able to restore their vision to some degree. This gives hope for patients with disorders like late-stage age-related macular degeneration, where the light-sensitive photoreceptor cells in the retina have already been completely lost. This type of research may also provide new treatments for people who suffer from retinal diseases like retinitis pigmentosa and glaucoma.
For direct repair of the retina, scientists are working to differentiate stem cells into working photoreceptors. These cells could be transplanted into the retina to replenish the retina with new photoreceptors, with the aim of restoring visual function. Several different techniques for this kind of transplant are being explored, including:
transplanting a full-thickness retina
transplanting 'sheets’ of photoreceptor cells
transplanting cells suspended in liquid growth medium (either photoreceptor cells, or capable of differentiating into photoreceptors)
transplanting a ‘sheet' of RPE photoreceptor cells
One of the interesting aspects of photoreceptor transplants is ‘material transfer’. This is where biological material, such as proteins, is transferred from the donor cells of the transplanted graft to the remaining host photoreceptors. Instead of truly integrating into the retina, these cells fuse with the existing photoreceptors. These fused cells and could potentially restore some visual function by 'rescuing' the remaining photoreceptors in the patient.
Several preclinical studies investigating these techniques are underway. It will be several years before we know the outcomes of these studies. These early efforts towards photoreceptor replacement therapy will assess their safety and tolerability in patients.
While the evidence of visual improvement in animal models is encouraging, this research is very much in its infancy. Several challenges remain to be solved, including
the optimisation of techniques for selecting and growing specific types of retinal cells
improving cell survival
developing techniques for delivering cells to the right area (particularly for cells requiring accurate alignment in order to integrate successfully into the host tissue)
Assessment of risks (such as the risk of tumour formation by undifferentiated stem cells, or prolific progenitor cells)
Current challenges
Challenges that remain in gene and cell therapy for eye diseases include:
precise delivery of cell to a specific region, while avoiding effects in other regions
improving immune response to transplanted cells, and appropriately assessing safety and efficacy
ensuring long-term durability of the desired effects
scaling up production while maintaining quality and affordability
ensuring accessibility of therapies to all patients.
Despite the highlighted challenges, research and technology advancements continue, moving us closer to effective treatments for eye diseases.
Collaboration between researchers, healthcare professionals, regulatory bodies, and industry stakeholders is crucial in overcoming these challenges and making these innovative therapies more accessible and effective for patients with eye diseases.
Next steps
Gene and cell therapy research holds immense promise for individuals living with vision disorders. The ongoing developments in the field could offer a transformative approach to treating vision loss, and improve the quality of life for those affected.
By harnessing the regenerative potential of stem cells, researchers are striving to replace damaged or lost retinal cells, including photoreceptors and retinal pigment epithelial cells. This groundbreaking therapy aims to halt disease progression, enhance visual function, and potentially reverse vision loss.
Early studies are underway to assess the safety and efficacy of transplanting stem cells and progenitor cells into the eye. Other hurdles to overcome include
improving protocols for selectively growing certain cell types
understanding and managing immune rejection of transplants
understanding human retinal development to fully understand what causes these diseases, and what processes need to take place to regrow healthy tissue
Although challenges remain, the future of stem cell therapy for visual disorders is bright. with the potential to revolutionize treatment options and bring new hope to those living with visual impairments.